
More than 20 years have passed since I flew to Madrid, Spain, to learn systematically about liposuction and mastered the live surgery course of the World Society of Dermatological Surgeons. Dr. Hankey and Dr. Satler, who were my professors at the time, became colleagues who frequently met at international conferences. At the time, we vehemently discussed the practical techniques for losing fat, and now we see that numerous new technologies - such as electric, laser, and internal/external ultrasound - have been developed since then. Now I think liposuction was not my only concern.
Ultrasonic liposuction machine has been developed through three significant steps. The first generation device was a method of dissolving fat with a rod-shaped probe diameter of 4 to 6 mm and then suctioning additionally with a hollow cannula. Then, in the mid-1990s, a second-generation device was released to perform both processes simultaneously: suctioning fat while generating ultrasonic waves from the cannula itself. Then, in 2001, the third-generation technology with a frequency of 36 kHz was presented with a titanium probe with a more precise diameter (2.2-4.5 mm) than existing equipment. And this latest device accomplished the theoretical development of ultrasonic liposuction.
The most crucial concept in medical devices is 'tissue selectivity,' which targets to damage only the desired tissue. Therefore, the most extensive development was creating a theoretical foundation for reducing selective adipose tissue; resonance with an ultrasonic wave close to 37-42 kHz, where fat is best dissolved, targets adipose tissue.
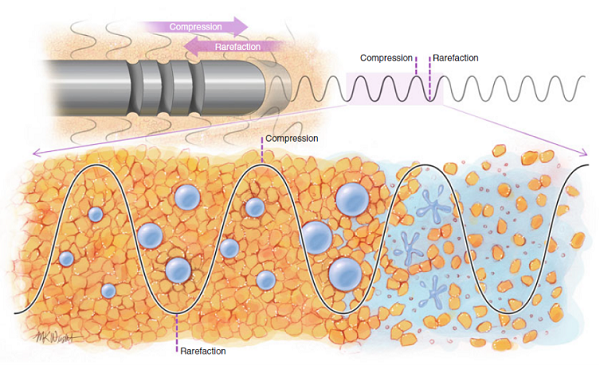
Among three significant interactions between this device and the tissue, the most important concept is 'cavitation'. For safe liposuction, when local anesthesia is performed with tumescent solution, Ultrasound waves are sent deep into the layers of your skin, causing a disruptive vibration with the probe moving back and forth repeatedly. And the tiny bubbles in the anesthetic solution get bigger and bigger, and eventually, these bubbles burst, breaking apart the surrounding fat cells. This technique is called cavitation and usually occurs within a few millimeters of the probe's tip, but it also occurs around minor grooves next to the probe.
The second interaction is the 'mechanical effect,' implying that reiterated contact has the consequence of physically destroying the tissue. And the third is the 'heat effect'. Repeated movement of tens of thousands of times per second will eventually generate frictional heat. Tissue changes caused by heat make the skin firm after the procedure and can also cause side effects such as burns, so you should always try to control this frictional heat. Moreover, it is also required to develop a needle with a smaller caliber for this purpose.
The thinner the probe, the less energy is transmitted. So the thinner probes allow fewer side effects due to heat, more sophisticated surgery, and minimized incision of the inlet. However, the problem is the probe manufacturing technology. In fact, out of a strong material called titanium, it is very complex to make a thin probe with a strong material called titanium because the probe must be strong enough to withstand tens of thousands of vibrations per second.
Elsa's 0.9mm probe, recently developed by New Pont, has the smallest diameter globally and is smaller than an 18G needle for blood collection. Thus this innovative technology allows surgery to be performed without incision and with only a minor injection mark. In addition, it is evaluated as an optimized device for stable procedures by applying the 'Deep Sono Algorithm' that tracks the frequency in real-time and keeps the output constant.
Reporter Han Jung-sun(fk0824@k-health.com) / Translated by Jini Jung
